
Scenario 6- Adnexa
1. Objectives
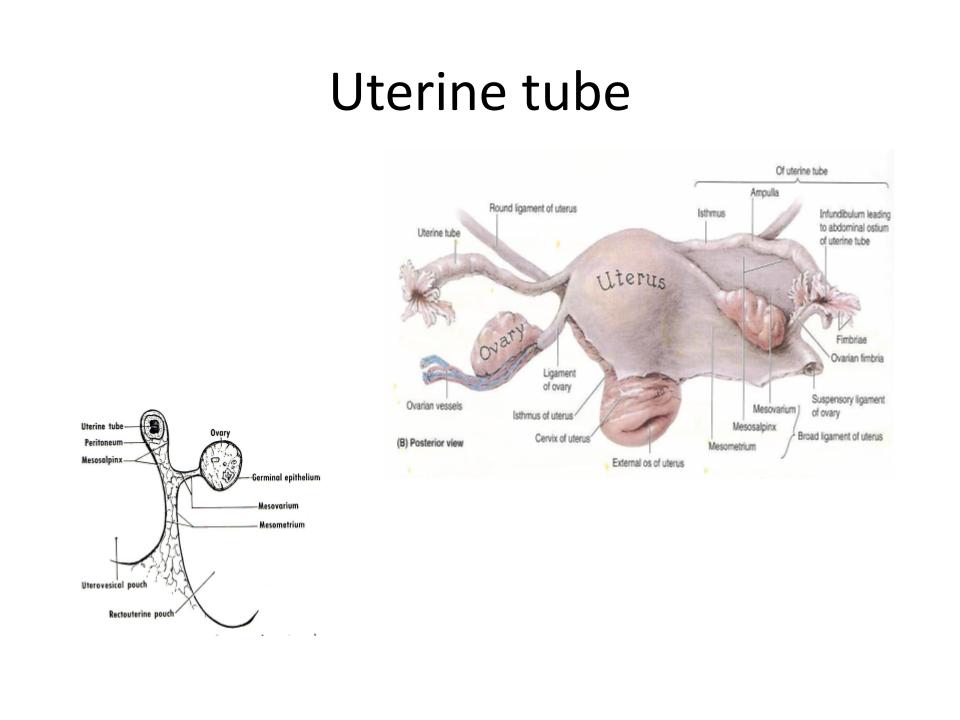
- Identify the 4 portions of the fallopian tube and describe their clinical significance.
- Identify the attachments of the ovary
- Describe the layers of the ovary
2. Relevant Anatomy
- Fallopian tubes- 4 portions of the fallopian tube
- Ovaries- Layers of the ovaries
- Attachments of the ovaries to the pelvis
3. Case 6
Ms. Tube is a 25 yo G1P0 with LMP 2 months ago and presents to the ER for severe right lower quadrant abdominal pain and vaginal bleeding. She has a positive pregnancy test. Pelvic ultrasound shows a 4 cm right adnexal mass with fetal cardiac activity and she is diagnosed with an ectopic pregnancy. She is taken to the operating room for a laparoscopic right salpingectomy.
3.1 You enter the abdomen laparoscopically and survey the abdomen. Identify the fallopian tubes bilaterally and name the four sections of the fallopian tube from proximal to distal.
{kind=link}
{kind=link}
3.1.1 What clinically relevant process occurs in the interstitial portion of the fallopian tube?
3.1.2 What clinically relevant process occurs in the isthmus of the fallopian tube?
3.1.3 What clinically relevant process occurs in the ampulla of the fallopian tube?
3.1.4 What clinically relevant process occurs in the infundibulum/fimbriated portion of the fallopian tube?
3.1.5 You visualize the right fallopian tube and there is a 4 cm purplish/red mass in the ampulla of the tube with a small opening in the tube that is bleeding. The surgeon decides to perform a right salpingectomy. Name and identify the structures the surgeon must incise to remove the right fallopian tube with the ectopic pregnancy?
3.2 We rarely remove an ovary in a 25-year-old patient, however, say you needed to remove her right ovary. Name and identify the attachments of the ovary that would need to be incised to remove the ovary.
3.2.1 Identify the ovaries bilaterally and identify+name the 2 layers of the ovaries and their function.
{kind=link}
– General information about the ovaries:
- The ovaries vary considerably in size between sides and between women.
- Ovarian fossa of Waldeyer– Ovaries lie in the upper part of the pelvic cavity and rest in a slight depression on the lateral wall of the pelvis between the divergent external and internal iliac vessels.
Why do we try to preserve the ovaries?
Which important structure runs near the Infundibulopelvic ligament that you want to avoid injuring when you are incising the IP?
-General information about the fallopian tube:
- The fallopian tubes vary in length from 8-14 cm
- The fallopian tube varies in thickness
- The narrowest portion of the isthmus measures 2-3mm in diameter
- The widest portion of the ampulla measures 5-8 mm in diameter
- The fallopian tube is composed of smooth muscle
- Inner circular layer
- Outer longitudinal layer
- In the distal portion of the tube, the layers are less distinct and near the fimbriated extremity, are replaced by an interlacing network of muscular fibers
- The epithelial lining of the tube is composed of ciliated columnar epithelium which beat in the direction of the uterus assisting in the transportation of the egg
- Fimbria ovarica– one projection, which is longer than the other fimbriae forms a shallow gutter that approaches or reaches the ovary
- Mesosalpinx– mesentery of the tubes contains the blood supply and nerves
- Arterial blood supply to the oviducts is derived from terminal branches of the uterine and ovarian arteries
- Fallopian tubes are innervated by parasympathetic and sympathetic nerves from the uterine and ovarian plexuses
- Sensory nerves are related to spinal cord segments T11, T12, and L1.