
1. Patient Complaint & History
Jane (gravida 1, para 0) and John have been trying to have a baby for a long time. They are delighted when Jane does a home pregnancy test and it indicates positive. She schedules an appointment, and she has come to the Obstetrics clinic for her first check-up and to confirm the pregnancy, approximately 8 weeks since she took the test.
2. Exam
First Trimester Testing
First-trimester screening is performed. Genetic Screening is undertaken.
A triple screen is performed including a maternal serum alpha-fetoprotein (MSAFP), beta human chorionic gonadotropin hormone (hCGH), and unconjugated estriol (uE3). An ultrasound was also performed.
3. Lab Results:
Although the estriol value is normal, Jane’s MSAFP is slightly elevated and at 3.0 MoM (3.0 Multiples of the median) and her hCGH level is 1200 mIU/mL (over 50% higher than expected for a single birth). An ultrasound shows that Jane has an amniotic fluid index (AFI) of 25 indicating early polyhydramnios <24). However, it is difficult to assess the ultrasound due to poor resolution.
Table 1. Reference blood markers and fetal condition.
| Condition | MSAFP | uE3 | HCG |
| Neural tube defect | Increased | Normal | Normal |
| Trisomy 21 | Low | Low | Increased |
| Trisomy 18 | Low | Low | Low |
| Trophoblast pregnancy | Low | Low | Very High |
| Multiple gestations | Increased | Normal | Increased |
| Stillbirth (fetal death) | Increased | Low | Low |
- In a normal pregnancy, between 28-32 days, the embryo is changing from a flat disk to a tubular structure.
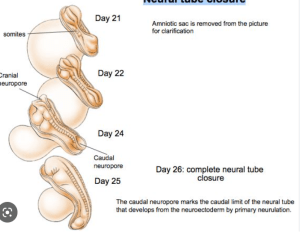
- By 28-38 days the normal embryo looks like this
4. Follow-up Appointment Tests
Upon presentation at a High-Risk clinic, an ultrasound performed denoted a single intrauterine pregnancy, polyhydramnios, anencephaly, and an omphalocele with ……… protrusion within the enclosed sac, measuring …. mm
5. Follow-up Results
A blood sample from Jane is obtained and a value of 380 ng/mL for alpha-fetoprotein (AFP, 0-40 ng/ML is normal) is determined. Normal serum levels of AFP are 10-20 ng/mL. Levels rise during pregnancy reaching a peak level at the end of the first trimester but they become diluted due to fetal blood volume increases. Substantial levels are found in 90% of neural tube defect cases.
An amniocentesis is scheduled to confirm an elevated level of AFP in the amniotic fluid.
The doppler indicates two heartbeats, indicating to the obstetrician that there are 2 babies, but there is a problem. Twin A is normal, but Twin B appears to have a major anatomical birth defect.
- Let’s review MRI scans of anatomical features.
Review osteology starting at the feet and ascending. Check lower limb bones; pelvis, and vertebral column. Then observe the cervical region and skull. Note deficiencies.
Model of the surface of the baby
Model of the skeletal system
A model of an encephalocele
- Schematic of a neural tube defect
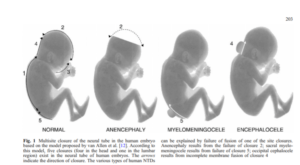
DeMarco et al., 2006 Neurogenetics 7:201-221
Model of a normal fetal skull
Segmented model of the brain
Photogrammetry specimen of a brain
Learning Objectives
-Describe the normal embryologic development of the anterior abdominal wall during the 4th to 5th week of development.
- Trilaminar Embryonic Disc
- Folding
-Explain what occurs during physiologic midgut herniation during the 6th week of embryologic development.
- Gut Formation
- Midgut development
-At how many weeks of embryologic development is midgut herniation no longer physiologic?
-Describe the 2 proposed mechanisms for the pathogenesis of omphalocele.
-Compare the differences between the major fetal abdominal wall defects- omphalocele and gastroschisis.
-Omphalocele may be associated with other birth defects. Recommend additional antenatal testing if a fetus is determined to have omphalocele.
-Develop a differential diagnosis for other birth defects that would affect the anterior abdominal wall. + How can they be differentiated?