

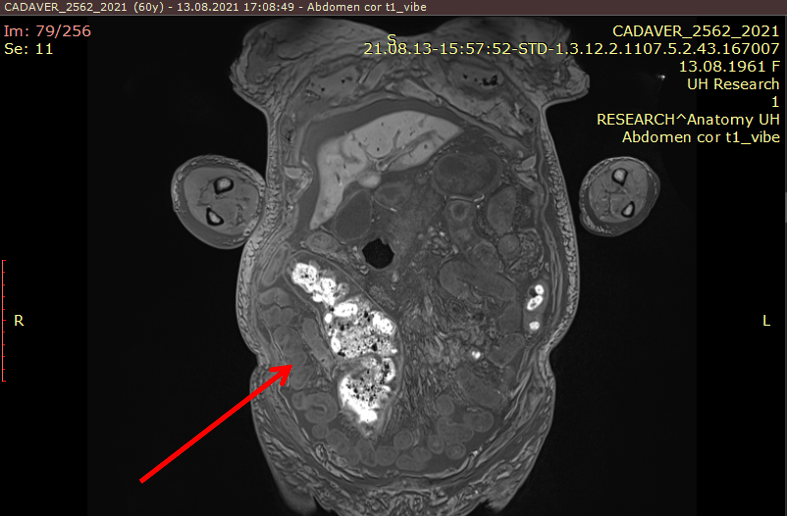
- You can see below small intestinal loops extending from the back of the descending colon to the right paracolic area
Definition
Protrusion of a bowel segment into another is called intussusception. A portion of the intestine inserts itself and gives the impression of a collapsing telescope. It produces severe abdominal pain and culminates in intestinal obstruction. In adults, intestinal obstruction due to intussusception is a relatively rare phenomenon, as it accounts for minority of intestinal obstructions in this population demographic. However, surgical resection without reduction is almost always necessary and is advocated as the best treatment for adult intussusception.
Radiology
CT is a modality of choice for assessment of acute abdomen in adults, and thus most frequently images intussusception. Also, short-length transient intussusception is a frequent incidental finding in MR. The appearance of intussusception is characteristic and depends on the imaging plane and where along with the bowel the images are obtained. Best known is the so-called bowel-within-bowel configuration, in which the layers of the bowel are duplicated forming concentric rings when imaged at right angles to the lumen, and a soft tissue sausage when imaged longitudinally.
Anatomical Considerations and Exercises
To locate and describe abdominal pain, it is necessary to understand the regionalization of the abdomen. The abdomen is characterized by a series of surface features related to the rectus abdominis and umbilicus. The linea alba forms as a median furrow separating the bilateral rectus abdominis muscles. Three tendinous insertions cross the rectus horizontally and serve to anchor this muscle to the rectus sheath. In some cases, such as pregnancy or a surgical incision, the bilateral rectus abdominis muscles will separate and a ridge-like elevation will occur in the midline. This condition is called diastasis recti and will be aggravated when intra-abdominal pressure is increased. The linea semilunaris is a laterally occurring furrow representing the lateral border of the rectus abdominis and sheath. See here the abdominal wall surface features.
The umbilicus may vary in position (usually at the level of L4) and is usually recessed; an everted umbilicus may suggest increased intra-abdominal pressure, perhaps from fluid in the peritoneal cavity (ascites). The umbilicus is used as a primary point for dividing the abdomen into quadrants, useful for descriptive purposes and you should trace these out visually and manually. A horizontal line through the umbilicus defines the transumbilical plane which usually intersects the intervertebral disc between vertebrae L3-L4. A vertical line bisecting the umbilicus, along with the horizontal line, divides the abdomen into a right upper quadrant (RUQ), left upper quadrant (LUQ), right lower quadrant (RLQ) and left lower quadrant (LLQ). The positions of the abdominal organs are often described in relation to these quadrants. An alternate system used for more accurate descriptions divides the abdomen into nine regions by the two midclavicular lines and two horizontal lines, one joining the lowest points of the costal margins (subcostal plane) and the other joining the tubercles of the iliac crest. Again, you should trace these nine regions visually and manually and designate them as (from superior to inferior and right to left): right hypochondriac, epigastric, left hypochondriac, right lumbar, umbilical, left lumbar, right inguinal, hypogastric (aka, suprapubic or pubic) and left inguinal regions. See abdominal regions here.
Also, use the picture below to draw the abdominal boundaries.
